PSA is much debated ...
There is a large overlap between PSA levels in people with and without prostate cancer
Despite years of study and testing and debate, we are left with the fact that we have no strong evidence that screening has a real impact. If anything, we have learned that screening certainly has more harms than people initially realized, with an excess number of cancers being detected and an excess number of men being treated without many of them benefiting from treatment. In this study, it is interesting that more high-grade cancers were detected in the control group, and that still didn't make a difference in mortality.
The bottom line is that after all these years, we need to make sure that people understand what we know and what we don't know about screening. What we know is that if there is a benefit, it's very small and it takes a long time to see it. Most of the men who are getting screened may not benefit and may have a risk of having unnecessary treatment, so better education is clearly important both for the primary care physician who is ordering the PSA test and for the individual man who is considering being tested. Hopefully, more information will be forthcoming, and at least men will get better information about what we know and don't know. Hopefully, we will stop giving a biased message about the overwhelming benefits of screening with PSA when we don't have any data that prove that to be the case.
The bottom line is that after all these years, we need to make sure that people understand what we know and what we don't know about screening. What we know is that if there is a benefit, it's very small and it takes a long time to see it. Most of the men who are getting screened may not benefit and may have a risk of having unnecessary treatment, so better education is clearly important both for the primary care physician who is ordering the PSA test and for the individual man who is considering being tested. Hopefully, more information will be forthcoming, and at least men will get better information about what we know and don't know. Hopefully, we will stop giving a biased message about the overwhelming benefits of screening with PSA when we don't have any data that prove that to be the case.
Digital Rectal Exam
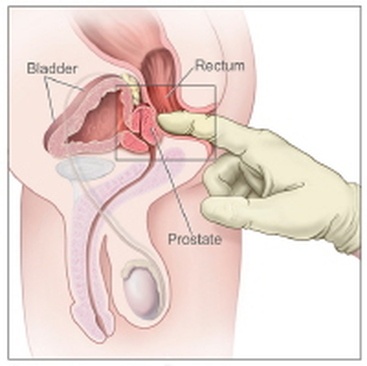
This might be able to detect cancer that starts in the back of the prostate. But if it starts just about anywhere else, it may miss it.
So the PSA is a recommended additional investigation.
And the DRE has other uses. It can pick up cancers of the anus and rectum.
So the PSA is a recommended additional investigation.
And the DRE has other uses. It can pick up cancers of the anus and rectum.
PSA Interpretation
PSA velocity
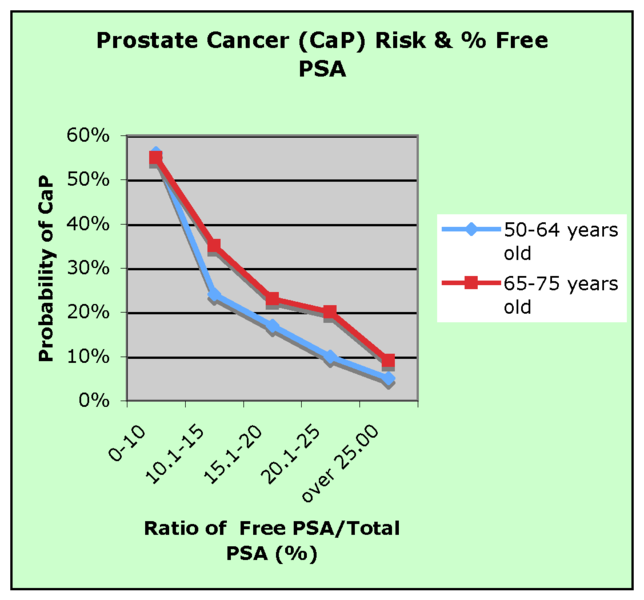
Risk of prostate cancer in two age groups based on Free PSA as % of Total PSA [32]
Despite earlier findings,[33] recent research suggests that the rate of increase of PSA (the 'PSA velocity') is not a more specific marker for prostate cancer,[34] e.g. >0.35 ng/mL/yr [35]
However, the PSA rate of rise may have value in prostate cancer prognosis. Men with prostate cancer whose PSA level increased by more than 2.0 ng per milliliter during the year before the diagnosis of prostate cancer have a higher risk of death from prostate cancer despite undergoing radical prostatectomy.[36]
Free PSA
Most PSA in the blood is bound to serum proteins. A small amount is not protein bound and is called 'free PSA'. In men with prostate cancer the ratio of free (unbound) PSA to total PSA is decreased. The risk of cancer increases if the free to total ratio is less than 25%. (See graph at right.) The lower the ratio is, the greater the probability of prostate cancer. Measuring the ratio of free to total PSA appears to be particularly promising for eliminating unnecessary biopsies in men with PSA levels between 4 and 10 ng/mL.[37] However, both total and free PSA increase immediately after ejaculation, returning slowly to baseline levels within 24 hours.[28]
Inactive PSA
The PSA test in 1994 failed to differentiate between prostate cancer and benign prostate hyperplasia (BPH) and the commercial assay kits for PSA did not provide correct PSA values. [38] Thus with the introduction of the ratio of free to total PSA, the reliability of the test has improved and measuring the activity of the enzyme could add to the ratio of free to total PSA and further improve the diagnostic value of test.[39] Proteolytically active PSA has been shown to have an anti-angiogenic effect [40] and certain inactive subforms may be associated with prostate cancer, as shown by MAb 5D3D11, an antibody able to detect forms abundantly represented in sera from cancer patients. [41] The presence of inactive proenzyme forms of PSA is another potential indicator of disease.[42]
Prostate Symptom Score, and then Prostate Cancer Risk Score
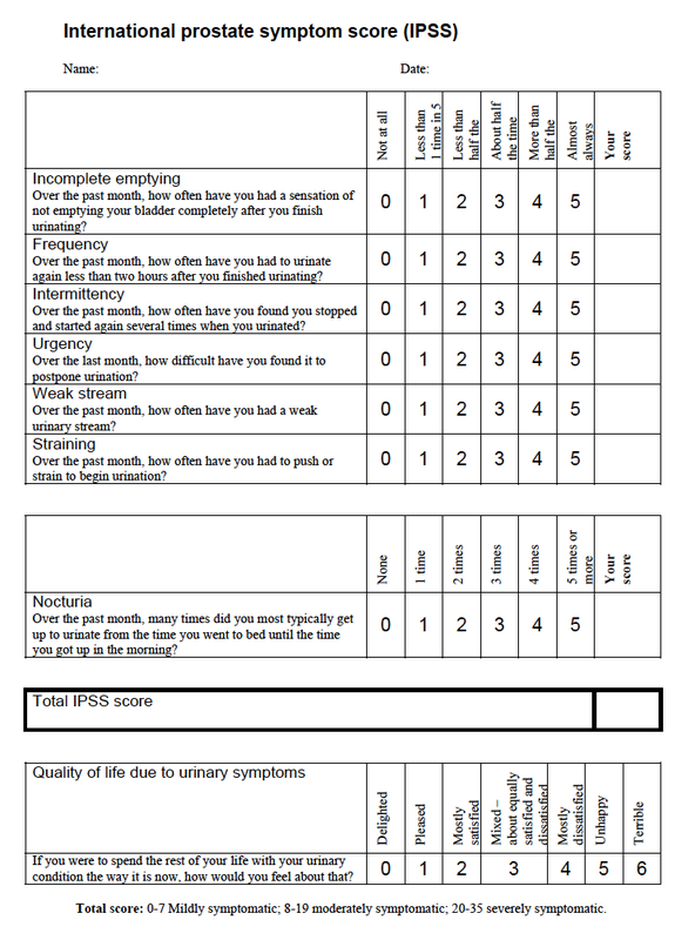
This is a score developed by Sunnybrook Hospital in Toronto to take into account all the latest information about what the risk factors for prostate cancer are.
First you need to fill out the International Prostate Symptom Score, (IPSS) which is the chart above.
Using this information, and other data you should have from your doctor, you can go to the web site and calculate your actual Prostate Cancer Risk Score.
The formula is not included in this page, but click on the link here and it will take you to the PROSTATE CA RISK CALCULATOR
First you need to fill out the International Prostate Symptom Score, (IPSS) which is the chart above.
Using this information, and other data you should have from your doctor, you can go to the web site and calculate your actual Prostate Cancer Risk Score.
The formula is not included in this page, but click on the link here and it will take you to the PROSTATE CA RISK CALCULATOR