Hi speed CT scanning for calcium in the coronary arteries

In an early study of autopsy findings in 2,500 patients, calcium in the coronary arteries and the total plaque burden were shown to be correlated. Patients who died of coronary artery disease were found to have 2-5 times as much calcium as those who died of other causes.
In June 2000, the American College of Cardiology (ACC) and American Heart Association (AHA) Consensus Panel wrote the following in the Journal of the American College of Cardiology: "Coronary calcium is part of the development of atherosclerosis; …it occurs exclusively in atherosclerotic arteries and is absent in the normal vessel wall." Simply put, the presence of calcification in the epicardial coronary arteries indicates that the patient has coronary atherosclerosis.[2]
This observation is of great significance, because atherosclerotic coronary artery disease is the number 1 cause of death in the Western world. Our ability to screen for coronary artery disease and, hopefully, prevent the sequelae of myocardial infarction and sudden cardiac death has traditionally depended on the assessment of atherosclerotic risk factors and on tests of coronary flow reserve.
Atherosclerotic risk factors have been evaluated in multiple longitudinal epidemiologic studies, such as the Framingham Heart Study. These studies have defined advancing age, male sex (or better stated, the absence of protective female hormones), hypertension, dyslipidemias, diabetes, cigarette smoking, and family history as predictors of subsequent cardiac events and angiographically demonstrated coronary artery disease.
Tremendous overlap exists, and sensitivities and specificities vary, even when multiple risk factors are applied. Novel risk factors have been proposed in an effort to enhance disease detection, particularly in asymptomatic patients. As a result, clinicians now may measure levels of homocysteine, fibrinogen, lipoprotein subunits (eg, lipoprotein A), C-reactive protein, and other biochemical markers of coronary atherosclerosis and subsequent cardiovascular events.
In June 2000, the American College of Cardiology (ACC) and American Heart Association (AHA) Consensus Panel wrote the following in the Journal of the American College of Cardiology: "Coronary calcium is part of the development of atherosclerosis; …it occurs exclusively in atherosclerotic arteries and is absent in the normal vessel wall." Simply put, the presence of calcification in the epicardial coronary arteries indicates that the patient has coronary atherosclerosis.[2]
This observation is of great significance, because atherosclerotic coronary artery disease is the number 1 cause of death in the Western world. Our ability to screen for coronary artery disease and, hopefully, prevent the sequelae of myocardial infarction and sudden cardiac death has traditionally depended on the assessment of atherosclerotic risk factors and on tests of coronary flow reserve.
Atherosclerotic risk factors have been evaluated in multiple longitudinal epidemiologic studies, such as the Framingham Heart Study. These studies have defined advancing age, male sex (or better stated, the absence of protective female hormones), hypertension, dyslipidemias, diabetes, cigarette smoking, and family history as predictors of subsequent cardiac events and angiographically demonstrated coronary artery disease.
Tremendous overlap exists, and sensitivities and specificities vary, even when multiple risk factors are applied. Novel risk factors have been proposed in an effort to enhance disease detection, particularly in asymptomatic patients. As a result, clinicians now may measure levels of homocysteine, fibrinogen, lipoprotein subunits (eg, lipoprotein A), C-reactive protein, and other biochemical markers of coronary atherosclerosis and subsequent cardiovascular events.
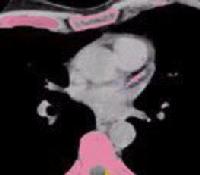
Pink means Calcium - Bad News !
The stress test has been used for many years to noninvasively identify coronary artery disease and to screen patients who are at risk for subsequent cardiac events. Although it is valuable in populations in whom atherosclerotic risk factors may produce obstructive coronary lesions, stress tests—even those performed with associated nuclear and echocardiographic imaging techniques—frequently fail in the identification of patients who are at risk for subsequent cardiac events.
Why does this testing sometimes fail? First, Bayesian analysis reveals that the usefulness of any test depends on the pretest likelihood of the presence of disease. Therefore, if stress testing is used in a population of asymptomatic individuals, it lacks both sensitivity and specificity, because the prevalence of obstructive coronary artery disease is low in this group. More important, the mechanism of cardiac events (ie, myocardial infarction, sudden cardiac death) is not detectible with the stress test or any measure of coronary flow reserve. Multiple angiographic and epidemiologic studies have shown that the mechanism of myocardial infarction and/or sudden cardiac death in asymptomatic patients is plaque rupture with superimposed thrombosis. In most cases, the plaque burden is not flow limiting; therefore, the patient does not have a positive stress-test result or even a significantly abnormal coronary angiogram.
These facts have renewed our interest in imaging techniques that can be used to detect a coronary atherosclerotic plaque at a point in its natural history when flow-limiting obstructive disease does not exist. Coronary calcification can begin in patients as young as 10-20 years. The calcification itself is calcium phosphate (hydroxyapatite), which is similar to that in bone. Such calcium deposition was believed to be the result of a degenerative process, but evidence now suggests an active process, perhaps a response to injury, that is regulated in the fashion similar to bone mineralization. At this point, the mechanism of calcium deposition in areas of atherosclerotic plaque is not completely understood.
Why does this testing sometimes fail? First, Bayesian analysis reveals that the usefulness of any test depends on the pretest likelihood of the presence of disease. Therefore, if stress testing is used in a population of asymptomatic individuals, it lacks both sensitivity and specificity, because the prevalence of obstructive coronary artery disease is low in this group. More important, the mechanism of cardiac events (ie, myocardial infarction, sudden cardiac death) is not detectible with the stress test or any measure of coronary flow reserve. Multiple angiographic and epidemiologic studies have shown that the mechanism of myocardial infarction and/or sudden cardiac death in asymptomatic patients is plaque rupture with superimposed thrombosis. In most cases, the plaque burden is not flow limiting; therefore, the patient does not have a positive stress-test result or even a significantly abnormal coronary angiogram.
These facts have renewed our interest in imaging techniques that can be used to detect a coronary atherosclerotic plaque at a point in its natural history when flow-limiting obstructive disease does not exist. Coronary calcification can begin in patients as young as 10-20 years. The calcification itself is calcium phosphate (hydroxyapatite), which is similar to that in bone. Such calcium deposition was believed to be the result of a degenerative process, but evidence now suggests an active process, perhaps a response to injury, that is regulated in the fashion similar to bone mineralization. At this point, the mechanism of calcium deposition in areas of atherosclerotic plaque is not completely understood.
Calcium Score is a very accurate predictor

Coronary segments with a luminal obstruction of greater than 50% are likely to have some calcification that is detectable with electron-beam CT (EBCT). In one trial, a 0 calcium score had a 100% predictive value in the exclusion of angiographic evidence of obstructive epicardial coronary lesions. The higher the calcium score, the more likely the presence of angiographic obstructive disease. In another study,[3] a calcium score greater than 371 had a 90% specificity in the detection of a luminal obstruction of greater than 70%. Specificity tends to decrease with advanced patient age, but it increases with the number of calcified vessels as well as the total calcium score.[4]
In a study in which calcium scores and thallium stress test results were compared, almost one half of the patients with scores greater than 400 had a normal thallium stress result.[5] Such testing may not be contradictory in terms of the pathophysiology; thallium detects inducible ischemia, not plaque burden.
Coronary calcification is strongly associated with the prognosis. Indeed, the extent of coronary atherosclerosis (total calcium score) is the most powerful predictor of subsequent or recurrent cardiac events. This was true in the early days when calcium was detected with fluoroscopy and conventional CT.
When EBCT calcium scores became available, the prognostic value of coronary calcification was again affirmed. The higher the calcium score, the worse the prognosis.[6, 7, 8] The degree of coronary calcium was a good predictor of the development of symptomatic cardiovascular disease. In a study by Agatston et al, the mean calcium score for patients with a cardiovascular event was 399, compared with a mean score of 76 in those without such an event. One study suggested that the detection of coronary calcification at EBCT was a better predictor of subsequent events than many traditional risk factors, including those evaluated in the Framingham database.[9]
Cardiac events do occur in patients with low calcium scores, but the incidence is low. Intravascular ultrasonographic studies show that as many 30% of coronary plaques are devoid of calcium. In an autopsy study,[10] the benefit of combined assessment of coronary artery calcification and risk factors (Framingham Risk Index) in predicting sudden cardiac death was apparent. In the study, 79 consecutive adults with sudden cardiac death were evaluated by using a Framingham Risk Index and histologic findings of coronary calcification. The risk classifications with the 2 techniques agreed in a majority of the patients. Patients with plaque erosion (as opposed to plaque rupture) who were dying of sudden cardiac death had significantly less coronary calcification and lower Framingham Risk Indexes.
Clearly, in establishing the cardiac risk, traditional coronary artery disease risk factors and coronary calcification may be most useful when used in combination. Whether risk stratification is further enhanced with the use of novel risk factors is yet to be determined.[6, 11, 12]
In a study in which calcium scores and thallium stress test results were compared, almost one half of the patients with scores greater than 400 had a normal thallium stress result.[5] Such testing may not be contradictory in terms of the pathophysiology; thallium detects inducible ischemia, not plaque burden.
Coronary calcification is strongly associated with the prognosis. Indeed, the extent of coronary atherosclerosis (total calcium score) is the most powerful predictor of subsequent or recurrent cardiac events. This was true in the early days when calcium was detected with fluoroscopy and conventional CT.
When EBCT calcium scores became available, the prognostic value of coronary calcification was again affirmed. The higher the calcium score, the worse the prognosis.[6, 7, 8] The degree of coronary calcium was a good predictor of the development of symptomatic cardiovascular disease. In a study by Agatston et al, the mean calcium score for patients with a cardiovascular event was 399, compared with a mean score of 76 in those without such an event. One study suggested that the detection of coronary calcification at EBCT was a better predictor of subsequent events than many traditional risk factors, including those evaluated in the Framingham database.[9]
Cardiac events do occur in patients with low calcium scores, but the incidence is low. Intravascular ultrasonographic studies show that as many 30% of coronary plaques are devoid of calcium. In an autopsy study,[10] the benefit of combined assessment of coronary artery calcification and risk factors (Framingham Risk Index) in predicting sudden cardiac death was apparent. In the study, 79 consecutive adults with sudden cardiac death were evaluated by using a Framingham Risk Index and histologic findings of coronary calcification. The risk classifications with the 2 techniques agreed in a majority of the patients. Patients with plaque erosion (as opposed to plaque rupture) who were dying of sudden cardiac death had significantly less coronary calcification and lower Framingham Risk Indexes.
Clearly, in establishing the cardiac risk, traditional coronary artery disease risk factors and coronary calcification may be most useful when used in combination. Whether risk stratification is further enhanced with the use of novel risk factors is yet to be determined.[6, 11, 12]